What is Lumbar Spine Disk Herniation and How Physio Can Assess or Treat it?
What is a Lumbar Disk Herniation?
The spine can be separated into 5 distinct levels, made up of 33 vertebrae. The cervical spine has seven vertebrae, the thoracic spine, twelve, the lumbar spine, five, the sacrum, five, and the coccyx, four. Although the sacrum and the coccyx collectively have nine bones, both groups are fused together to make two large bony structures. Therefore, the lumbar spine is the lowest truly mobile section of the spine. 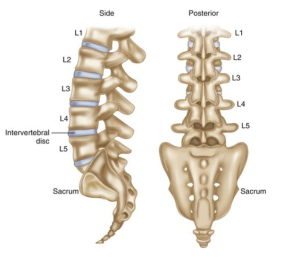
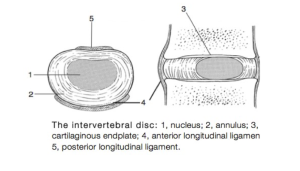
The vertebrae are separated by vertebral disks. Disks are made up of a thick outer layer, made up of fibrocartilaginous connective tissue called the annulus fibrosus. Within this is a softer, gelatinous substance called the nucleus pulposus, largely made up of type II collagen and water. Together they provide a buffer that supports movement and absorbs and distributes forces.
Either side of the disk runs two ligaments that extend the whole length of the spinal column, called the anterior and posterior longitudinal ligaments, supporting the disk and vertebral bodies. The posterior is roughly half as thick as its anterior counterpart, meaning the likelihood of herniations affecting the posterior is greater.
When the spinal column and disk are subject to extreme forces, the annulus fibrosus can tear, allowing the nucleus pulposus to push through the cartilaginous outer structure. This is known as a disk herniation and can range from partial to complete.
Who gets lumbar spine disk herniations?
Largely speaking, most people will experience a disk herniation. A study by W.Brinjikji (2015) looked at a group of healthy, pain free individuals. Using imaging and scans they assessed each one for spinal conditions. Their results showed that 30% of people over 20 years old had lumbar disk bulges, 50% over 40 and 69% over 60. All without any pain. This means that often people will experience a disk herniation, without knowing, or an experience of pain.
However, let’s look at who is most likely to experience a painful episode of disk herniation. A recent systematic review and meta-analysis showed the following risk factors were associated with higher likelihood of lumbar disk herniation .
- Smoking/history of smoking – it is hypothesised that the reason for this is due to the toxins released through smoking, ultimately leading to slower healing times, reduced disk nutrition and oxygenation, and reduced expression of collagen matrices.
- Diabetes – changes that occur on a cellular level in those that suffer from diabetes have been shown to potentially increase susceptibility to prolapse and following prolapse, healing times may be slower and less robust.
Additional potential risk factors included age, gender and occupation. However, the papers collected in this study did not illustrate sufficient data to confirm these claims (Huang W, 2016).
It is also important to differentiate between risk factors and causal factors. These two risk factors highlight variables that may increase the likelihood of a disk herniation. However, they are not likely to be the event that causes a disk herniation. Often, the causes of herniation include bending, lifting and twisting movements, sudden impact forces on the spinal column,
How common are disk herniations?
Herniations are relatively common, as discussed previously. On average, herniations will occur in between 0.05 to 0.2 per 100 persons. It is most common in people between the 3rd and 5th decade and typically affects males and females on a 2:1 ratio. In those aged between 25 and 50, the likelihood of a disk herniation affecting the L4-S1 region is 95%.
What are the Common Signs and Symptoms?
Common signs and symptoms of disk herniations are as follows:
- Pain at the region of the spine
- Radicular symptoms may be present in the leg. The pattern of which depends on the level of herniation.
- L4 – Typically back pain radiating into the anterior thigh and medial lower leg
Dermatomes – Sensory loss to the anterior thigh and sometimes medial lower leg
Myotomes – ankle dorsiflexion weakness
Reflex – Decreased patellar reflex.
- L5 – Typically Back pain, radiating into buttock, lateral thigh, lateral calf, and pinky toe
Dermatomes – Sensory loss on the lateral calf, pinky toe
Myotomes – Weakness on toe extension and flexion, foot eversion
Reflex – Decreased semitendinosus/semimembranosus reflex.
- S1 – Typically Back pain, radiating into buttock, lateral or posterior thigh, posterior calf, lateral or plantar foot
Dermatomes – Sensory loss on the posterior calf, lateral or plantar aspect of foot
Myotomes – weakness of plantar flexors of the foot. Additionally, Urinary and fecal incontinence as well as sexual dysfunction.
Differential Diagnoses
- Discal cyst – A very rare form of growth located on the intervertebral disks, commonly causing lower back discomfort and radicular pain into the leg. (Aydin, Sabri et al., 2010)
- Synovial cyst – Also a rare form of cyst affecting all levels of the spine, typically causing radicular pain and neuro deficits. (Khan, Amir M, 2006)
- Degenerative spinal stenosis – Spinal stenosis refers to the narrowing of the spinal canal, caused by bone deposition (stenosis). This may also result in neurological symptoms and pain similar to disk herniation.
- Metastasis – metastasis refers to a cancerous growth that has spread, or metastasized. Such growths can form on the vertebrae causing them to become weak, brittle and painful. (Fares J et al., 2020)
- Osteophytes – osteophytes are bony growths, typically formed in conditions such as osteoarthritis or spinal stenosis. These bone ‘spurs’ can irritate the surrounding tissues, causing swelling and discomfort.
- Cauda equina syndrome (CES) – CES is a serious time critical condition, typically resulting in symptoms such as saddle area anaesthesia, disruption to the bladder and bowel and bilateral leg symptomology.
Assessments/Tests
What Makes it Worse?
- Pain may be provoked by bending and twisting movement
- Palpation on and around the area
- Symptoms may worsen with prolonged activity or sitting
- Symptoms can often worsen at night or first thing in the morning
- Straightening the leg on the affected side
What Do People Tell Us?
History in these patients should include chief complaints, the onset of symptoms, where the pain starts and radiates. History should include if there are any past treatments.
People may describe:
- Pain may be present at the back, but may also travel up the back and down into the legs
- Stiffness at the back and legs
- Possible loss of function (strength, control, sensation) in more severe cases
- Onset of pain may be gradual/spontaneous or part of a significant event
- You may have trouble sleeping, especially when twisting in bed
What Do We Find on Physical Assessment/Testing?
Visual
The patient may be bracing the injury by holding their bodies in a certain way. This may result in an altered gait or slow, tentative movements. The patient may be forced to make adaptations to their daily activity such as not being able to sit comfortably or may not be able to sit at all.
Palpation (touch/pressure)
Palpation of the area and surroundings may be sensitive and painful. They may guard the area and not allow you to touch it.
Range of motion (Movement available at the joint)
Range of motion is likely to be reduced at the area of injury. For instance, if the disk bulge is posterior lateral on the left side, back extension and left side flexion is likely to be painful and therefore not allow a normal range of movement.
Strength
Strength may be reduced for a number of reasons.
- Strength may be limited by painful range of movement
- Strength may be reduced due to neurological tissue damage
- Bracing required to complete strenuous activities may increase the intra abdominal pressure, increasing pain symptomatology.
Special tests
- Straight leg raise (SLR) compared to asymptomatic leg
Conservative Treatment
Physiotherapy treatments that a physio may offer you:
Advice regarding PEACE/LOVE protocols
A physiotherapist is educated on the principles that surround the peace and love protocols and are therefore in a position to pass this knowledge onto patients in a way that they can understand.
In the acute stages of injury the following actions are recommended:
- Protection
- Elevation
- Avoiding anti-inflammatory drugs (not applicable in some situations)
- Compression
- Education
Followed by the following in the more chronic stages:
- Loading Optimally
- Optimism
- Vascularisation
- Exercise
This evidence based protocol was developed by Blaise Dubois and Jean-Francois Esculier for the BJSM in 2019, as a tool to follow on from acronyms such as RICE, PRICE or POLICE. Obviously, there are some aspects of the peace and love principles that cannot be applied to lower back pain, such as elevation. However, the full paper breaks down each aspect individually, most of which are applicable to lower back pain.
Manual therapy
Mobilisation and manipulation movements can be used to aid in pain relief and range of motion in the short term. NICE guidelines recommend the consideration of manual therapy (spinal manipulation, mobilisation or soft tissue techniques such as massage) for managing low back pain with or without sciatica, but only as part of a treatment package including exercise, with or without psychological therapy.
Acupuncture
Practitioners such as Geoff Maitland and Ronald Melzack have long practised the notion of counterirritation and localised microtrauma. Acupuncture is one form of this methodology that aims to increase activity and blood flow to the local area, promoting healing. The theory behind it is multifactorial, one of which proposes that localised noxious stimulation at the injury site activates the descending inhibitory systems, reducing nociceptive transmission to the brain from the level of the spinal cord, relieving pain. This process is mediated by the enkephalin group of endogenous opiates, released at spinal and supraspinal levels (Fields et al 2006).
Strapping, taping and bracing
Strapping, taping and bracing are all forms of external support that can be used to protect the area, aid in movement, and act as a sensory reminder of the injured structure whilst the area recovers. It is well known that strapping, taping and bracing can be used as a valuable adjunct tool in the physiotherapists arsenal, especially in the acute stages of an injury. However, such intervention should not be considered as a sole treatment option (Nelson NL et al., 2016).
Advice on anti-inflammatory agents and creams
Although PEACE/LOVE protocols advise against the use of anti-inflammatory agents in the acute phase of injury, in some cases, the need for a reduction of inflammation is great. The medium in which anti-inflammatory aids can vary depending on the nature of the inflammation and therefore advice on which to use may vary from person to person. This may include topical creams, oral tablets or even supplements rich in natural anti-inflammatories such as curcumin, often ingested for anti-inflammatory effects at a dose of about 5 g/day.
Advice on supplements for injury recovery
In addition to this, advice may be provided on nutrient intake, such as the increased demand for protein, up to 2.2g/kg (that’s a lot!) when injured, or the benefits of creatine monohydrate supplementation, for lean muscle mass and strength retention during periods of forced inactivity. Both have been researched heavily, both display excellent safety profiles (Rawson, E. S. et al., 2018).
Equip you with specialist equipment, such as foam rollers, bands, etc.
In addition to educating and prescribing a treatment approach, a physio is able to equip the individual with all the necessary equipment for their rehab journey. This may include resistance equipment, orthotics, braces, matts or mobility aids, making the process fluid and simple.
Home exercises that can help – V = check out our YouTube for example videos!
Stretching
- Back extensions – extensions aim to reduce pain and increase function. Begin in prone lying. If tolerable, aim to push down onto your hands, causing the back to curve into extension. Maintain contact with the ground through the hips.
- Pelvic rocking – pelvic rocking is a movement completed in supine lying, the person shifts their tailbone into anterior and posterior pelvic tilt. This aims to increase strength, mobility and control of the upper, mid and lower spine and pelvis.
- Lying Knee Drops – starting in supine lying with their ankles and knees together and legs bent to 90 degrees, actively drop the legs to one side applying rotation at the lumbar vertebrae, whilst maintaining both shoulders on the ground. This will open up the facet joints of the spine and aims to decrease pressure on the disk, nerve root or other symptomatic structures.
Exercises you may progress towards as you become stronger:
- Bridging – With the patient in supine, bridging requires the participant to segmentally mobilise the spine by lifting the sacrum, lumbar, lower thoracic, mid thoracic and upper thoracic spine off the ground, building strength and control of all these sections.
- Cat/camel – Similar to bridging, cat/camel requires segmental control of the spine. This time in four-point kneeling, the individual aims to arch the spine into anterior pelvic tilt, maximal extension of the spine and neck, before rounding the spine, through posterior pelvic tilt and complete flexion of the spine. With this movement, the participant can build mobility and control.
- In addition to this, various pilates-based exercises may be used to build strength, control and mobility at the back and spine, such as:
| Matt Work | |||
| Position | Action | Benefit | |
| ‘Bird Dog’ | Four point kneeling | Raise contralateral arm/legs keeping the core muscles contracted | Erector spinae, glute, scapula stabiliser and deltoid muscles |
| ‘Dead Bug’ | In supine with their arms straight up and their knees and hips at 90 degrees of flexion (upside down four point kneeling) | Lower contralateral arms and legs, maintaining contraction at the core | Hip flexor, transverse ab, pelvic floor muscles |
| ‘Spine Corrector’ | Supine, sat on the equipment. | Slowly bend backwards, achieving passive extension at the lumbar and thoracic spine | Spine mobility and flexibility into extension |
| Trapeze Table | |||
| Starting Position | Action | Benefit | |
| ‘Prone Scapula Slides/ Back Extension’ | prone lying, holding onto arm bar | Shrug the shoulders down into retraction and depression, whilst keeping the arms straight. For extension, then add cervical/thoracic spine extension. | the postural muscles – lat, rhomboids, erector spinae, rot cuff |
| ‘Spread Eagle Standing’ | standing, holding onto frame, feet on frame | Keeping the legs straight, allow the pelvis to drop back, bringing the back into spinal flexion. Then bring the pelvis to base, bringing the spine into extension. | Building strength in the grip, control of the shoulder girdle, segmentation of the spine and range of motion available at the hip and ankle. |
| ‘Hamstring Stretch 1’ | standing with one leg on the floor, the other on the trapeze | maintaining a straight back, hip hinge forward towards the raised leg, stretching the hamstring | Elongating the muscles and nervous tissue in the hamstring and lower back |
| Multi Chair | |||
| Starting Position | Action | Benefit | |
| ‘The Mermaid’ | Seated, on the multichair. | Remaining seated, long reach up and abduct the arm over the body, lateral flexing at the spine | Lengthening the side of the body. (obliques, QL, Glute??, TFL??) |
| ‘Back extensions’ | Laying prone, on the multi chair. Hands on foot plates | Using the foot plates for assistance, actively bend the spine upwards, extending the spine | Assisted contraction of the back extensors, lengthening of the back flexors |
| ‘Rotations’ | Laying prone, on the multi chair. Hands on foot plates. | Using the foot plates for assistance, actively rotate the spine, allowing one arm to lift, whilst the other remains firm. | Assisted rotation of the lumbar spine, unilateral extensor activation and stretching of the obliques?? |
| Reformer | |||
| Starting Position | Action | Benefit | |
| ‘Circles both ways’ | Lying supine on the reformer with lower legs in ankle straps. | Lifting the lower limbs, hips remain grounded. Control the lumbosacral junction. Complete small circles with the legs in both directions. | Control of the lumbosacral junction, hip and core musculature. |
| ‘Prone Spine Extension’ | Lying prone on a box on the reformer, with hands on the foot bar | Press the foot bar away with the arms, extending the neck, upper and then lower thoracic spine. | Strengthening, mobilising and building control of the scapula stabilising, mid/upper back and neck muscles. |
| ‘Bridging’ | Lying supine on the reformer, with feet on foot bar | Pushing down on the foot bar with the feet, lift the tail bone, lumbar, lower thoracic and then mid thoracic spine off the reformer pad. Hold, then return to base. | Glute and hamstring strengthening, increased control r.e. segmentation of the spine. |
Evidence for this form of exercise in groups experiencing LBP
Exercise modalities that focus more closely on core muscle activation, such as pilates, are commonly used as a first line of treatment in the management of those with lower back pain pathologies. The use of core activation and strengthening exercises for the treatment of lower back conditions is a widely discussed topic.
Previously, lower back pain was often associated with reduced firing rate of the core musculature. Hodges PW and Richardson CA. (1996) were the first to research core muscle activation in those suffering from lower back pain. In their study they state
“The delayed onset of contraction of transversus abdominis indicates a deficit of motor control and is hypothesised to result in inefficient muscular stabilisation of the spine”.
Since then, more recent research has shown that training to increase core muscle firing rate is ineffective in reducing pain levels (Vasseljen O et al., 2012). In addition to this, another study looked at populations who had recovered from lower back pain and found that their firing rate had not changed, suggesting that the rate of firing is not a causal factor in the experience of pain (Moreside JM et al., 2014).
In more recent years, modern science has shifted to adopt a ‘biopsychosocial outlook’ on the experience that is pain, one that cannot simply blame misfiring muscles, but rather casts a greater emphasis on the emotions, experiences and dynamic interactions that precede the onset of pain. Nevertheless, this does not mean that core activation and strengthening exercises are not beneficial in the treatment of lower back pain.
One study by Eliks M et al. (2019) highlights the positive effect that clinical pilates can have on instances of lower back pain. In their study they found that both matt and equipment based exercises can provide therapeutic benefits to pain and function. More specifically, their findings showed optimum results when completed in a class format, led by an instructor, for around 60 minutes, 2-3/per week. In addition to this, another study by Jill A Hayden et al. (2021) aimed to explore which exercise type was the best for treating lower back pain pathologies. In which they concluded that the use of both mckenzie and pilate based movements were shown to be superior to other activities such as yoga, aerobics, and rest.
An earlier systematic review and meta-analysis by Xue-Qiang Wang et al (2012) found that core activation exercises, something pilates bases many of their exercises from, are “more effective in decreasing pain and may improve physical function [when compared to general exercise].” However, they also found that these benefits were primarily apparent in the short term. In the longer term, the inter-group differences became less significant.
To summarise, pilates is one method for the implementation of total body and core strengthening. There is a wide base of support for the use of and effectiveness of this form of exercise in populations suffering from lower back pain. Benefits are especially seen in the short term, providing an argument for their usage in the acute stages. In the long term, exercise type becomes less important.
Key Take-home Messages
1: The cause of LBP is multifactorial, and therefore there is no ‘one size fits all’ approach to management
2: Pain/symptoms are generally experienced in the lower back, buttocks muscle and occasionally down the leg (depending on the level of injury)
3: The spine, discs and the surrounding structures are extremely strong in nature, and therefore with the correct management/advice, this condition can be managed conservatively
4: Physiotherapy treatment including mobilisation, acupuncture, bracing and exercise prescription are all effective in the management of LBP
5: Strength and Flexibility exercise, whether it be at home or in Pilates, are proven to be effective in long term management of LBP
References:
Aydin, Sabri et al. “Discal cysts of the lumbar spine: report of five cases and review of the literature.” European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 19,10 (2010): 1621-6. doi:10.1007/s00586-010-1395-9
Dubois B, Esculier J. Soft-tissue injuries simply need PEACE and LOVE. British Journal of Sports Medicine 2020;54:72-73.
Eliks M, Zgorzalewicz-Stachowiak M, Zeńczak-Praga K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: state of the art. Postgrad Med J. 2019;95(1119):41-45. doi:10.1136/postgradmedj-2018-135920
Fares J, Fares MY, Khachfe HH, Salhab HA, Fares Y. Molecular principles of metastasis: a hallmark of cancer revisited. Signal Transduct Target Ther. 2020;5(1):28. Published 2020 Mar 12. doi:10.1038/s41392-020-0134-x
Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine (Phila Pa 1976). 1996 Nov 15;21(22):2640-50. doi: 10.1097/00007632-199611150-00014. PMID: 8961451.
Huang W, Han Z, Liu J, Yu L, Yu X. Risk Factors for Recurrent Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Medicine (Baltimore). 2016;95(2):e2378. doi:10.1097/MD.0000000000002378
Jill A Hayden, Jenna Ellis, Rachel Ogilvie, Samuel A Stewart, Matthew K Bagg, Sanja Stanojevic, Tiê P Yamato, Bruno T Saragiotto. Some types of exercise are more effective than others in people with chronic low back pain: a network meta-analysis. Journal of Physiotherapy, vol. 67,4 (2021)1836-9553
Khan, Amir M, and Federico Girardi. “Spinal lumbar synovial cysts. Diagnosis and management challenge.” European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 15,8 (2006): 1176-82. doi:10.1007/s00586-005-0009-4
McFarlin, Brian K., et al. “Reduced inflammatory and muscle damage biomarkers following oral supplementation with bioavailable curcumin.” BBA clinical 5 (2016): 72-78.
Moreside JM, Quirk DA, Hubley-Kozey CL. Temporal patterns of the trunk muscles remain altered in a low back-injured population despite subjective reports of recovery. Arch Phys Med Rehabil. 2014 Apr;95(4):686-98. doi: 10.1016/j.apmr.2013.10.003. Epub 2013 Oct 15. PMID: 24139985.
Nelson NL. Kinesio taping for chronic low back pain: A systematic review. J Bodyw Mov Ther. 2016 Jul;20(3):672-81. doi: 10.1016/j.jbmt.2016.04.018. Epub 2016 Apr 27. PMID: 27634093
Rawson, E. S., Miles, M. P., & Larson-Meyer, D. E. (2018). Dietary Supplements for Health, Adaptation, and Recovery in Athletes, International Journal of Sport Nutrition and Exercise Metabolism, 28(2), 188-199. Retrieved Jun 17, 2022, from https://journals.humankinetics.com/view/journals/ijsnem/28/2/article-p188.xml
Vasseljen O, Unsgaard-Tøndel M, Westad C, Mork PJ. Effect of core stability exercises on feed-forward activation of deep abdominal muscles in chronic low back pain: a randomized controlled trial. Spine (Phila Pa 1976). 2012 Jun 1;37(13):1101-8. doi: 10.1097/BRS.0b013e318241377c. PMID: 22146280.
Wang XQ, Zheng JJ, Yu ZW, Bi X, Lou SJ, Liu J, Cai B, Hua YH, Wu M, Wei ML, Shen HM, Chen Y, Pan YJ, Xu GH, Chen PJ. A meta-analysis of core stability exercise versus general exercise for chronic low back pain. PLoS One. 2012;7(12):e52082. doi: 10.1371/journal.pone.0052082. Epub 2012 Dec 17. PMID: 23284879; PMCID: PMC3524111.